Adhesive Capsulitis
Olecranon Stress Fracture
The patient is an elite baseball pitcher who felt progressive pain in the posterior aspect of his elbow during fall ball. He presented with a stiff shoulder, a diminished arc of motion, and deficiencies in his core musculature. X-rays demonstrated an olecranon stress fracture (far right xray – red arrow). He was shut down from throwing and began to work in physical therapy for his range of motion deficiencies. At two months, the stress fracture showed progression of healing (middle image). By three months, his olecranon stress fracture had healed and he was allowed to begin an interval throwing program (far left xray – red arrow). He returned to pitching at an elite level.
- Photo 1


Hook of the Hamate Fracture
The patient is an elite level baseball player who noticed increasing wrist pain while taking batting practice. Finally, with one swing he felt a pop. X-rays were within normal limits. MRI and CT scan both demonstrated a fracture at the hook of the hamate. The red arrow indicates the fractured hamate on the MRI scans. Given the small size of the bony fragment, surgery involves merely excising the fragment. Surgery is necessary to remove the pain associated with the fragment that is too small to heal and sees such great forces with the swinging of a baseball bat. The patient returned to gripping exercises by week 3 and returned to baseball at week 6 post operative.
- Photo 1

- Photo 2



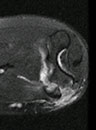
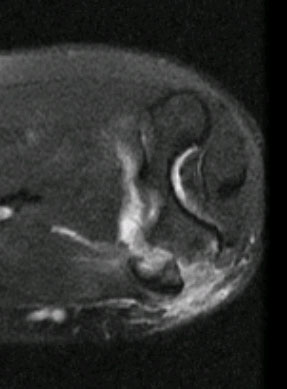
UCL Thumb
The patient is an elite level baseball player who injured his thumb while sliding into second base head first. Physical exam demonstrated UCL laxity. X-rays showed no fracture. MRI demonstrated a high grade injury to the UCL of the MCP joint. In photo 1, the yellow arrow denotes the torn UCL and the orange arrow denotes the adductor policis brevis muscle which blocks the healing of the UCL. Photo 2 demonstrates the ligamentous instability at the MCP joint with volar subluxation. Surgery is necessary to restore the normal anatomy and relationship of the ligament in relation to the tendon. The patient returned to gripping exercises by week 3 and returned to baseball at week 6 post operative.
- Photo 1

- Photo 2



Medial Epicondyle
The patient is an elite HS baseball pitcher who felt a "pop" to the inside of his elbow while throwing a fastball. X-rays showed that he avulsed the medial epicondyle growth center off of the humerus (photo 1). The MRI shows that the bony fragment contains the attachment of the common flexor origin, portions of the growth plate, and the ulnar collateral ligament – aka the tommy john ligament (photos 2,3). Surgery was performed to reduce the avulsed bony fragment with a single screw and repair the ulnar collateral ligament (photos 4,5). Progressive healing occurs over the next 8 weeks and by 12 weeks the player returns to throwing (photos 6,7).
- Photo 1

- Photo 2
- Photo 3

- Photo 4

- Photo 5

- Photo 6

- Photo 7







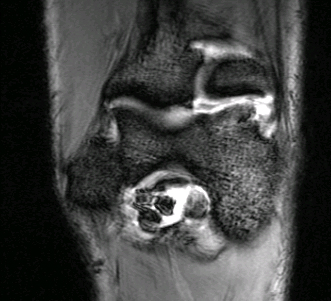
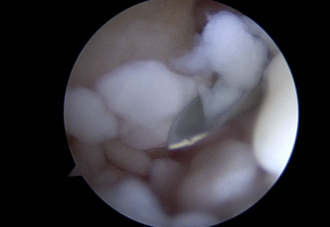
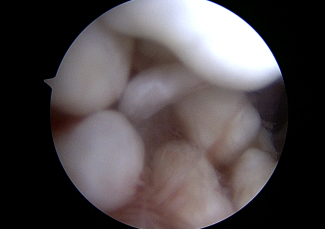
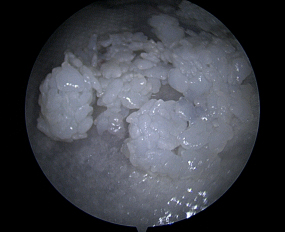
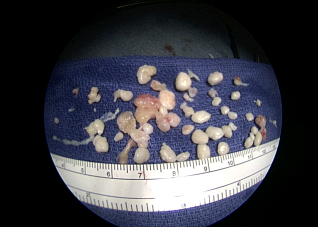
Synovial Chondromatosis of the Elbow
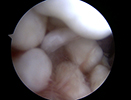
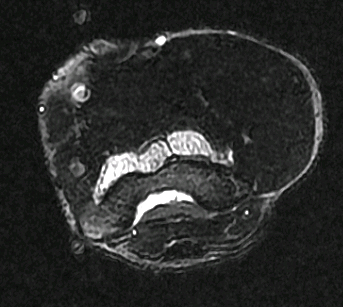
The patient is a 40 year old recreational athlete who presents with catching, locking, and swelling to his elbow. He has also experienced a loss of motion gradually over the last few years. MRI (photo 1,2,3) demonstrates loose bodies that were “too numerous too count” according to the radiologist’s report and consistent with the diagnosis of synovial chondromatosis – a benign condition. The patient underwent arthroscopic surgery of the elbow and the numerous loose bodies were seen and removed (Photo 4,5,6). The pieces ranged in size from that of a grain of a rice to a pea (Photo 7,8). The patient returned to cross fit and his regular workout regime within 6 weeks.
- Photo 1

- Photo 2
- Photo 3

- Photo 4
- Photo 5
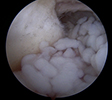
- Photo 6
- Photo 7
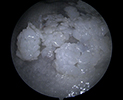
- Photo 8



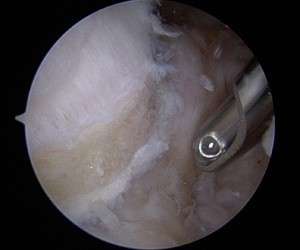
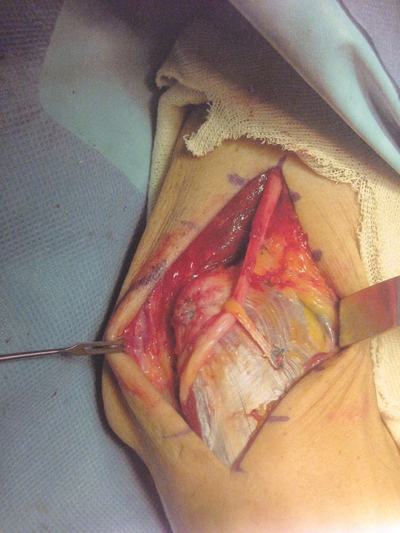
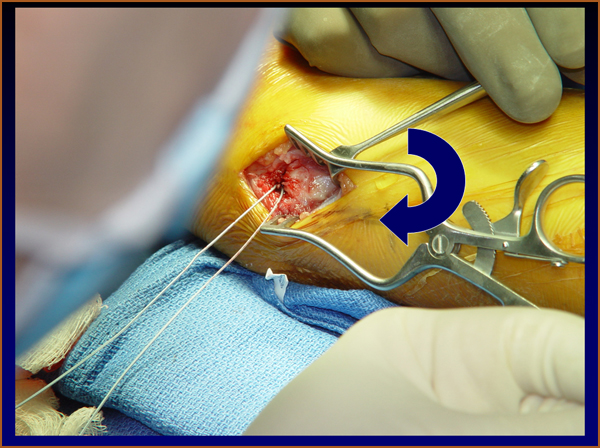
Common Extensor Origin Debridement and Reattachment
Patient is a middle aged male who has 18 month history of lateral side elbow pain. He initially felt a pop while lifting weights. He continued to weight train and had a steroid injection, but the pain persisted. He then came to see Dr. Shepard for a second opinion where MRI revealed a full thickness tear of the common extensor origin. The patient elected to undergo open common extensor debridement and reattachment .
- Fig 1
- Fig 2
During the surgery, a lateral incision is made and dissection is done to the level of the CEO.
- Fig 3

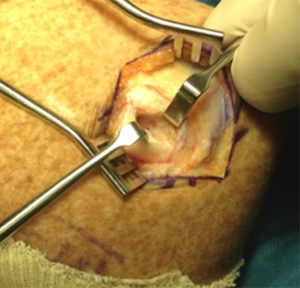
The dead tissue is debrided and removes then the healthy bone is scrape to stimulate bleeding to aid in the healing process. Anchors are placed in the bone and stitches are place through the remaining healthy tissue. This tissue is then secured to the bleeding bone.
- Fig 4

- Fig 5



- Fig 6


Following the surgery, the patient is instructed to do no heavy lifting or repetitive grip activity for 6 weeks. Initially the goal of rehab is to focus on range of motion. At the six week mark, the patient can begin a strengthening program. Patient is released to full activity at the three month mark.
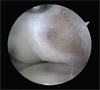
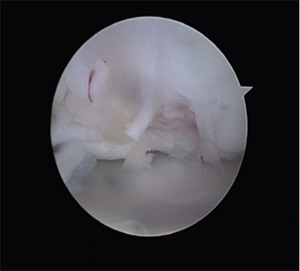
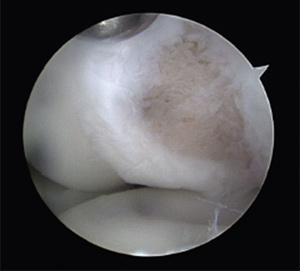
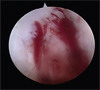
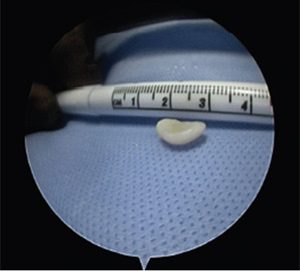
OCD Lesion with Micro Fracture of the Elbow
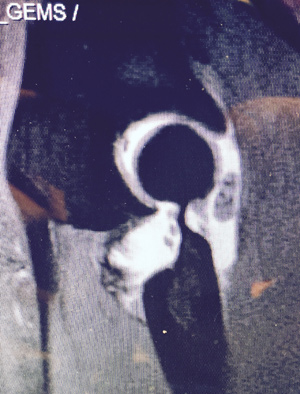
Patient is an 11 year-old-female who is a competitive gymnast. She had persistent right elbow pain and limited range of motion. An MRI revealed an 8mm x 6mm x 2mm slice of cartilage off the central portion of the capitellum. The radial head was intact.
- Fig 1

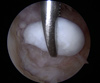
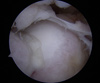
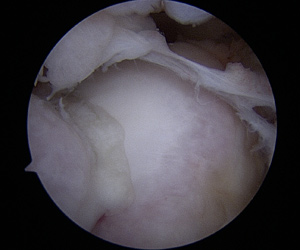
The patient and her family elected to undergo arthroscopic removal of the loose body and microfracture of the capitellum in hopes of regenerating healthy cartilage in the area of the OCD lesion.
- Fig 2

- Fig 3
- Fig 4


- Fig 5
- Fig 6


Valgus Extension Overloard.
An elite level pitcher with a painful bonespur off of the tip of the olecranon is removed arthroscopically with a high speed bone cutter. The patient experiences posterior elbow pain with terminal extension. The MRI shows multiple loose bodies and a bone spur off of the olecranon tip. The arthroscopic pictures show the loose body and the picture of the olecranon after excison. The video shows the removal of the bone spur.
- Fig 1

- Fig 2

- Fig 3
- Fig 4

Right Elbow Arthroscopy - Michael Shepard MD
Patient is an active 55 year old male with persistent pain to the inside of his elbow and instability to his ulnar nerve
Patient is an active 55 year old male with persistent pain to the inside of his elbow and instability to his ulnar nerve. After failing conservative therapy the patient elected to undergo debridement and repair of his common flexor origin in addition to subcutaneous ulnar nerve transposition. Figure 1 is the patient's MRI which demonstrates the tearing at the medial epicondyle where the common flexor origin attaches to the humerus. Figure 2 demonstrates the hole or tearing in the common flexor origin at the time of surgery – this tear was debrided and then reattached to the humerus with the use of a suture anchor. Figure 3 shows the final surgical result with the ulnar nerve transposed.


Valgus Extension Overload in a Professional Pitcher
The patient is a 26 year-old professional baseball player with increasing pain with follow through. He presents with pain in the medial aspect of the posterior compartment. His exam is consistent with classic valgus extension overload. His MRI demonstrates loose pieces posteriorly along with a large posterior medial osteophyte (MRI1 and MRI2). Arthroscopic pictures reveal two large loose pieces in the posterior compartment of the elbow (AS1, AS2). The large posterior osteophyte was loose and the source of his pain with pitching (AS3, Phyte video). The loose fragments and osteophyte were removed (AS4). The tip of olecranon was resected as well to decrease pain with terminal extension / follow through. (AS5) The patient returned to pitching at 6 weeks post operation.
- MRI 1

- RI 2

- AS 1

- AS 2

- AS 3
- AS 4
- AS 1



Phyte Video
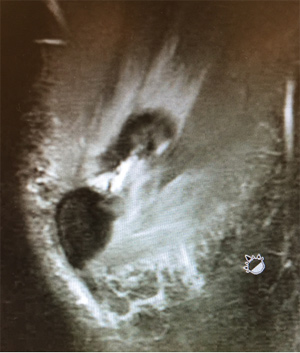
Ulnar Stress Fracture
Patient is an 18-year-old college baseball player with chronic elbow pain when throwing. On x-ray exam, it was found the patient’s elbow demonstrated a chronic stress fracture of his olecranon process (ulna). After failure of conservative management including extensive physical therapy, the patient and his family elected to undergo right elbow open reduction internal fixation with a tension band and with a takedown of the non union.
X-rays were taken two months after surgery and they show near complete resolution of the stress fracture. Patient was able to resume elite level of baseball.
- Picture 1

- Picture 2

- Picture 3

- Picture 4




Medial Epicondyle Avulsion Fracture:
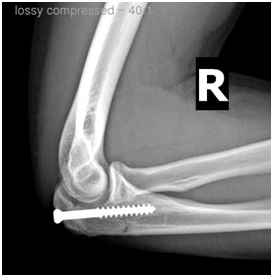
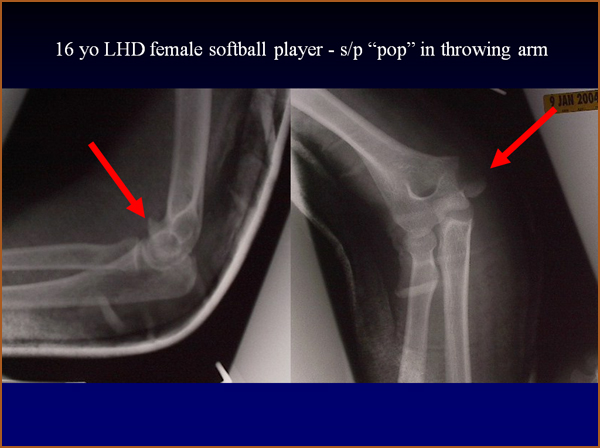
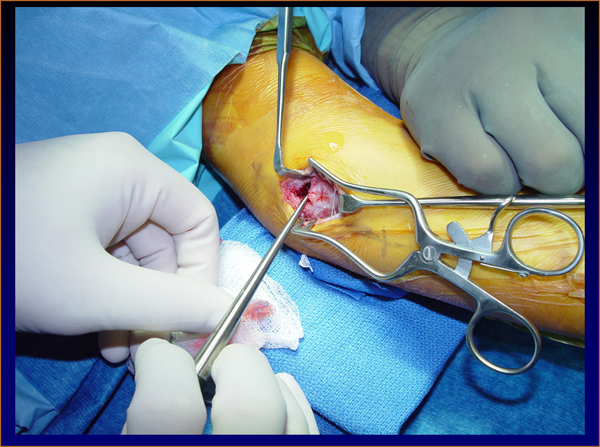
The patient is a 16 year old softball athlete who felt a pop while throwing to 1st base. She has avulsed her medial epicondyle via the pull of the mediall epicondyle. At surgery, the ulnar nerve was decompressed, but was not transposed. A suture is place around the common flexor origin to get control of the fracture fragment. A 4.5 mm screw is inserted into the medial epicondyle to hold it in its anatomic position while it heals. She returned to unrestricted softball in 3 months and played for another 4 years at the collegiate level without difficulty.
Click on the thumbnails for enlarged view


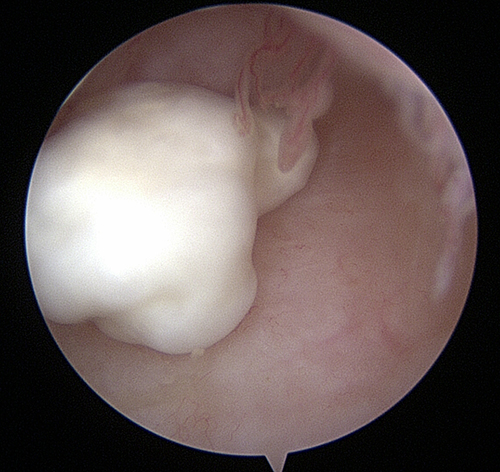
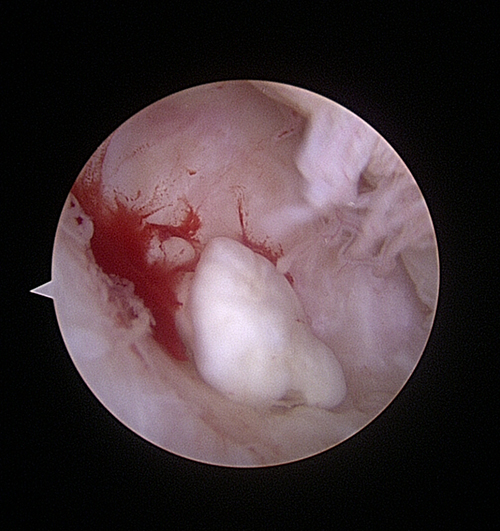
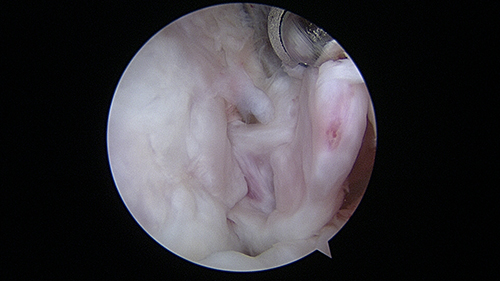
Arthroscopic Elbow Arthrofibrosis Release
Arthrofibrosis (stiff joint) is a common reason people come to see Dr Shepard. Using four to six poke holes in the skin and a combination of cameras (2.7 mm, 4.5mm), Dr Shepard will remove the loose bodies, bone spurs, and the contracted capsule (casing) that restrict the elbows range of motion. Less than 10% of Orthopaedic Surgeons perform elbow arthroscopy and even fewer perform arthroscopic releases. An arthroscopic release caries several advantages over traditional open releases: less pain, quicker recovery, better final range of motion.
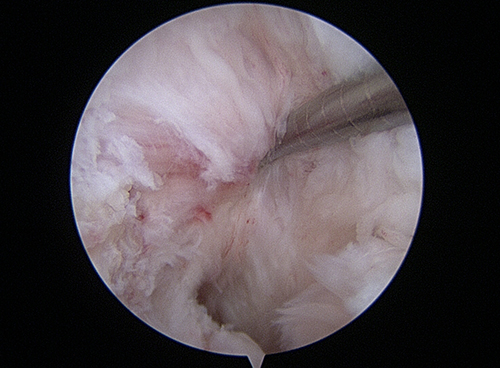
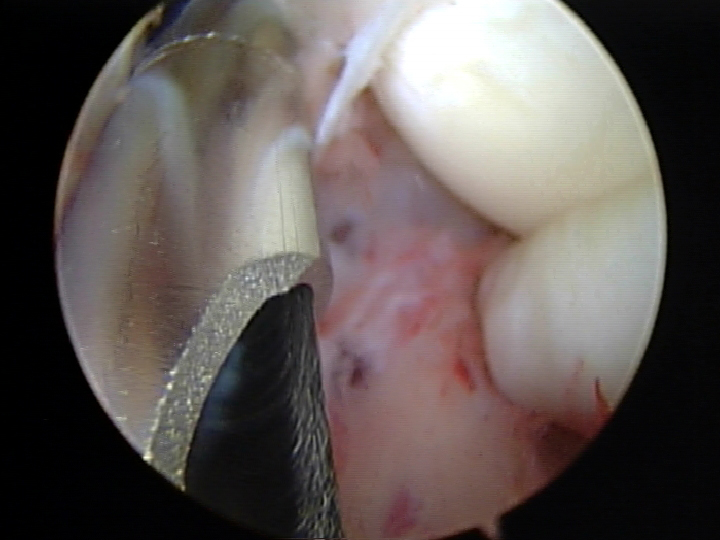
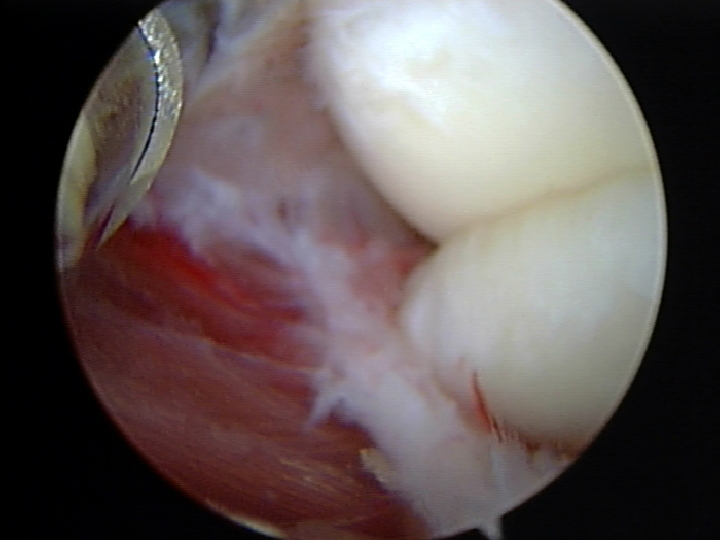
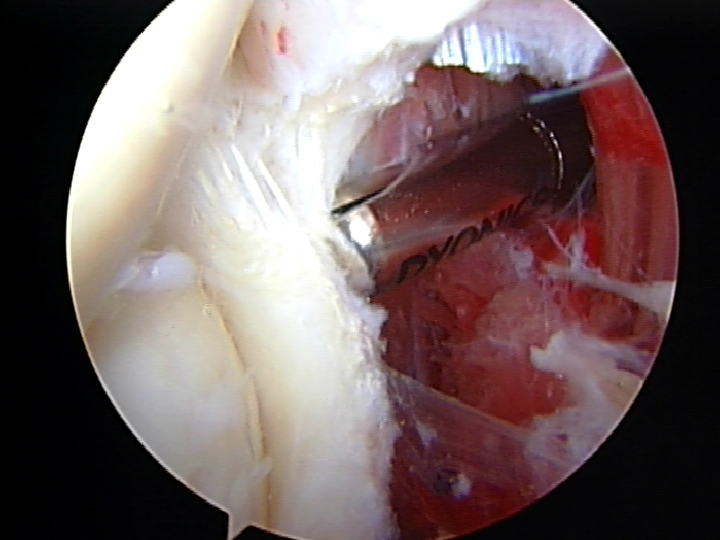
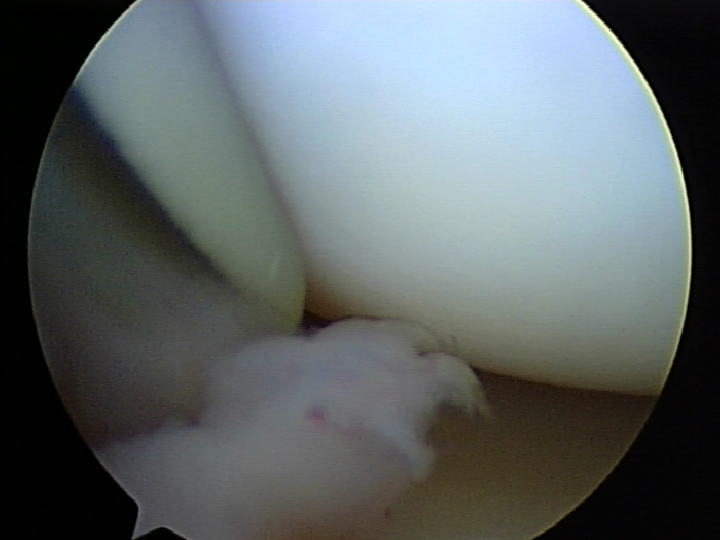
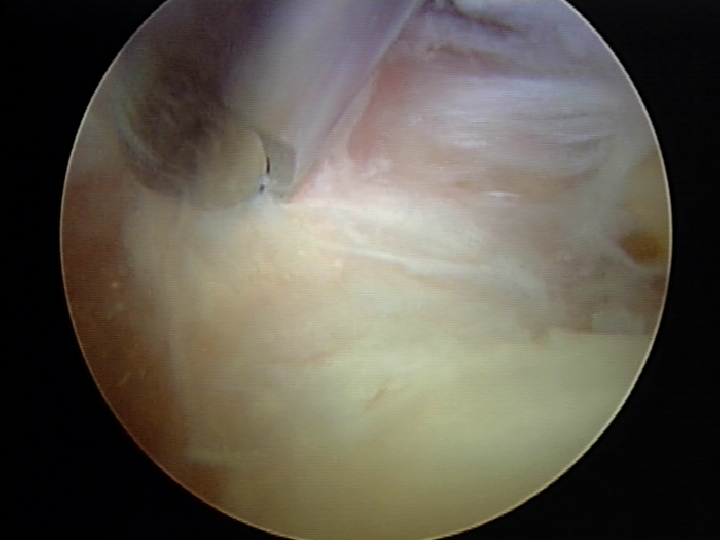
This patient presented with severe loss of motion - her range of motion was 30-95 degrees, whereas normal motion is 0 (straight) to 145 (bent) degrees. Picture 1 shows the scarred anterior capsule, which was restricting extension. Pictures 2, 3 and videos 1,2 show the anterior capsule being resected. Picture 4 shows the removal of a loose body that was causing irritation and pain. Pictures 5,6 and video 3 show resection of the olecranon tip / bone spurs and the resection of the posterior capsule. Final motion achieved with the release was 0-135.
Click on the thumbnails for enlarged view
- Picture 1

- Picture 2
- Picture 3

- Picture 4
- Picture 5

- Picture 6


Video 1
Video 2
Video 3
Subcutaneous Ulnar Nerve Transposition
Ulnar Nerve Transposition is performed for irritation of the ulnar nerve in the cubital tunnel and or recurrent subluxation of the nerve out of the tunnel. In this patient, the nerve was unstable during simple elbow range of motion and while playing water polo.
Video 1
An incision is made directly over the medial epicondyle - allowing access to the nerve proximally in the arm between the brachialis and the triceps, as well as access distally as the nerve enters the forearm. Care is taken during the dissection to isolate the medial antebrachial cutaneous nerve which runs across the incision. A wide dissection is neccessary to adequately decompress the nerve.
Video 2
The nerve is idenitifed proximal to the medial epicondyle and protected with a vessel loop. Distally, the nerve penetrates the two heads of the flexor carpi ulnaris muscle and this muscle is carefully split to allow decompression and transposition of the nerve.
Video 3
The ulnar nerve is transposed out of the cubital tunnel and lays atop the common flexor origin. A sling is fashioned from the fascia overlying the common flexor origin to gently prevent recurrent subluxation. Finally, the triceps fascia is reapproximated to the cubital tunnel to "close the tunnel" and ensure the nerve could not fall back into the tunnel.
How is elbow arthroscopy different than other surgeries?
Elbow arthroscopy is not as common a procedure as arthroscopy of the knee and shoulder. According to the American Academy of Orthopaedic Surgeons Survey, less than 10% of orthopaedic surgeons perform elbow arthroscopy. Elbow arthroscopy is technically demanding, requires multiple portals, utilizes multiple cameras, and should be performed with someone with a strong background in the surgery. Dr Shepard learned elbow arthroscopy from world famous James R Andrews MD – one of the developers and forefathers of the technique in the United States. Dr Shepard has performed elbow arthroscopy on high level overhead athletes from UC Irvine, Cal State Fullerton, and Chapman Universities.
Who needs elbow arthroscopy?
There are two primary groups of people who undergo elbow arthroscopy – young overhead athletes with loose bodies and OCD lesions; older people with loss of motion (arthrofibrosis).
The young athletes often develop loose bodies or cartilage lesions from their repetitive injuries. These lesions can be treated through the arthroscope with loose body removal and cartilage restoration techniques. These injuries are most commonly seen in baseball and softball athletes, as well as young athletes who compete in gymnastics, wrestling, and weight lifting.
The older athlete who looses motion, also known as arthrofibrosis, can be treated through the arthroscope as well. These patients loose the function of their elbow as their motion decreases over time. This problem can be treated with an arthroscopic release of scar tissue and capsule to restore motion. Sometimes, a small burr will be used to resect bone spurs to restore motion.









